Since the advent and commercial availability of Sildenafil Citrate in 1998, (known throughout the world to one-and-all as Viagra ®), the market for treatments for erectile dysfunction has grown to become worth about $2 billion worldwide per annum. That is now projected to grow to $4 billion per year by the year 2004 and to an astonishing $6 billion per year by 2006! (1)
Results of recent surveys indicate that, on average, 15% of the male population has suffered from erectile dysfunction. As a strong indicator of its age-related increase, more than 50% of men over the age of 60 have varying degrees of erectile dysfunction (ED). So it may not be surprising that it is estimated that ED affects approximately 31 million men in the United States, and as a whole, there may be as many as 300 million men around the world suffering with ED! (1)
Therefore, to cash in on this huge and relatively new market, (at least in terms of its acceptance), it is no surprise to discover that numerous pharmaceutical companies are rushing to find new drugs and new methodology, to treat this sexual disease that is clearly an age-related disorder.
That is the subject of this article, we shan’t get too bogged down in the psychology of impotence, or the social or economic impacts of such a “disease” and its treatments. What we shall concern ourselves with here are the pharmacokinetics, uses, interactions, effects and properties of these revolutionary new approaches to erectile dysfunction.
In order for us to ascertain the difference between the new treatments for ED when compared to Viagra ®, it is first necessary to remind ourselves of the properties of Pfizer’s stock market winner.
Viagra ® is rapidly absorbed by mouth with a bio-availability of about 40% and peak concentrations of the chemical are in the blood within 30-120 minutes. (2) This has been one of the advantages for Viagra ®, in that it is capable of being taken as a tablet and is relatively quick-acting. A convenient factor when perhaps one’s partner won’t wait forever!
The affects of Viagra ® will last, on-average, for up to 4-hours and its metabolites are excreted in the faeces and urine. Viagra ®’s affect is to inhibit an enzyme known as phosphodiesterase type-5 (PDE5), which naturally occurs in erectile tissue. PDE5 can break down cyclic GMP, the substance that is produced during sexual arousal and causes vascular and muscular changes that eventual lead to an erection. (2)
Therefore, men who produce too little cyclic GMP have problems obtaining and maintaining an erection, and men who produce too much PDE5 have problems obtaining and maintaining an erection.
Viagra ® is well known to be contraindicated with organic nitrates. These are drugs that are often used to treat heart conditions such as hypotensive conditions, (low blood pressure). Viagra ® appears to potentiate the effects of nitrates and therefore the two must not be taken concurrently. Furthermore, caution is advised for any patient using Viagra ® who has a heart problem, even if they are not using nitrates for the condition. (2)
Viagra ® dosages are usually 25mg to 100mg (50mg doses being the average), taken up to one hour before sexual intercourse. These dosages have produced side effects such as headache, flushing and dyspepsia. There have been some reports of disturbances, dizziness, and nasal congestion. Other rarer adverse effects reported include diarrhea, muscle pain, skin rashes, and urinary or respiratory-tract infection. (2)
Viagra ® undoubtedly represents a very significant advance in the treatment of erectile dysfunction, but like most drugs it is not without its cautions, contraindications and potential side effects etc.
Alprostadil is a drug that has been available for the treatment for ED years before Viagra ® was even a twinkle in the eyes of the pharmacologists at Pfizer. Yet alprostadil has all but disappeared as a front line treatment for ED, this is despite the fact that some clinical trials indicate that alprostadil is as effective as Viagra ®! So why would that be?
There is one simple answer, it was because of alprostadil’s delivery method, but as we will learn, all that is about to change.
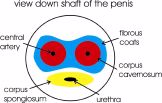
Alprostadil is a hormone like substance that is referred to as prostaglandin E1, a known and potent vasodilator (improver of blood flow). Alprostadil has the power to directly effect the tissue that it comes into contact with. (3) An erection essentially occurs when the blood vessels widen in the genital region and allow the corpus caverosum (Figure 1) to fill with blood, and hence the penis becomes erect and stiff. So, it is easy to see the direct role that alprostadil plays in the creation of an erection.
Figure 1
Originally, alprostadil was used to treat neonates with congenital heart defects. In order to treat this condition, alprostadil has to be directly injected into the heart region. (4) This is the same drug that is used to treat ED, and until very recently the delivery method was the same principle! In other words, brand name products such as Caverject ® were injected into the flaccid tissue of the penis with fast acting results. Having spoken to some who have practiced this method, it is apparently quite painless, but the thought of having to place a needle into one’s vital member is undoubtedly a “bridge too far” for most men! When one considers that this is meant to take place prior to love making, the two concepts/ thoughts just don’t seem to go together!
Muse ® was another development of alprostadil that tried to reduce the psychological aspects of the Caverject ® delivery method. In essence, alprostadil was produced in intraurethral pellets; tiny tablets that can be inserted down into the eye of the penis with the aid of a minute insertion stick. But once again, the prospect of the delivery method, is still too much for most men, to consider it to be a worthwhile regular method of treatment for ED.
I think one can easily understand why Viagra ® tablets have taken the world by storm!

Alprostadil: The Recent Development
But that may now all change with the concept of an alprostadil cream. Known as Befar ®, (it may also be released later in some countries under the trade names of Alprox ® and Topiglan ®), this is the first topical cream in the world for the treatment of ED.
Currently, only commercially available in the Far East, Befar ® has shown a clinical efficacy of up to 83% in patients with varying degrees of ED. (6) The cream itself has a onset action of 10-15 minutes and can continue on past 4-hours, (Figure 2) and is favorably comparable to the efficacy of the injectable alprostadil. (3, 19)
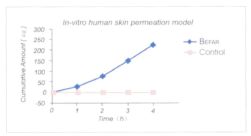
Figure 2
Due to Befar’s direct application method (i.e. unlike Viagra ®, Befar’s actions are limited to the area of its application), the side effects induced by the application have to date been limited to transient warm and burning sensations.
So instead of using an injectable or intra-urethral pellet, Befar ® cream rapidly and effectively promotes the permeation of alprostadil into the active site of the penis.
In one randomized, double-blind, placebo-controlled, multi-center clinical trial conducted in China (5), 157 ED patients aged 26 to 75 with various etiologies (psychogenic, organic and a combination of both), had an mean average ED history of 5-years. They all received treatment of Befar ® or a placebo for 4-weeks. After the 4-week period, the Befar ® patients improved their ability to have and maintain their erections by 68%, (it’s noted as Primary Efficacy on Figure 3). The same patients also improved the frequency and strength of their erections by 75%, (it’s noted as Global Efficacy on Figure 3). As can be seen on the same bar graph, this was a very significant difference over placebo.
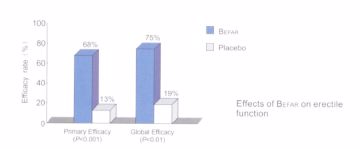
Figure 3
Since then, another trial conducted in a 303 patient phase II clinical study in the United States has shown an impressive efficacy rate of 83% (6) Other clinical trials support similar results. (7)
During these trials, the side effects noted have been mild urethral pain, a feeling of urethral burning, penile fullness and redness at the application site. Most of the adverse events were mild and transient and all naturally resolved in a short time, without requiring any medical treatment.
Below, the chemical structure of alprostadil.
Surprisingly, Befar ® may also be suitable for women too! One study, suggested that its data supported further investigation for topical alprostadil in the treatment of Female Sexual Arousal Disorder (20). For whist ED is now a recognised disorder, clitoral stimulation by vasodilatation is beginning to be seen as an important aid to sexual satisfaction for women.
If there is a disadvantage to Befar ®, it may be the fact that it is very temperature sensitive. It is strongly recommend that Befar ® (and for that matter all alprostadil creams), remain in a fridge at a temperature of 2 to 8 degrees Celsius. The manufacturer claims that Befar ® may be kept at up to 25 degrees Celsius for up to 14-days (8), but it is clear that any temperature in excess of that can wreak the active ingredient within hours, perhaps even minutes if the temperature is higher still. It would appear that when temperature damage occurs that the product takes on a clear look, rather than its normal strong white creamy appearance. Once damaged by heat, Befar ® has no active ingredient and hence no action.
So the shipment of Befar ® to-and-from the patient and its compulsory storage conditions may be its weak-point, but from the pharmacological and medical viewpoint Befar ® is clearly a major improvement over its earlier rivals.
Apomorphine has been available as a drug for many years, but the first thing that we should clear up, is that even though it has the word “morphine” contained within its name, apomorphine is different to morphine, and has no morphine like affects. (2, 9) For example, where morphine is a sedative, apomorphine is a stimulant. As such, apomorphine does not have any of the affects associated with that narcotic.
Above, the chemical structure of apomorphine.
In the few countries where apomorphine is currently commercially available, (those being Australia, France, Italy, Netherlands, New Zealand and the United Kingdom), it is not a controlled substance. (2, 9, 10, 11, 12, 13)
Apomorphine is used in the control of Parkinson’s disease. Specifically, for the senile dementia, it is delivered as a subcutaneous injection and it is used for Parkinson’s because it is a dopamine agonist. In other words, it improves the levels of the neurotransmitter that is most affected in Parkinson’s disease.
Later, it was noticed that Parkinson’s patients were regularly having penile erections after their injection. These were clearly being induced by the apomorphine and it was soon realized that the drug may have an additional medical role. (14) Unsurprisingly, it wasn’t long before it came to the attention of a pharmaceutical company. The first to bring an ED treatment containing apomorphine to the market, was Abbot Laboratories of the United Kingdom. Their development of a sublingual tablet, under the trade name of Uprima ® is causing a great deal of interest.
Uprima ® is a potent agonist of dopamine, specifically it acts upon D1 receptor sites, and this makes it different to the majority of ergot derived drugs for dopamine improvement, such as, bromocriptine, which normally target D2 receptors. (21) Accordingly, Uprima ® doesn’t act directly upon the penis like Viagra ® or Befar ®, but instead exerts its influence in the brain for arousal, pleasure and climax. Uprima ® is known to act upon receptors in the hypothalamus, and that this can enhance erection by increasing the signals from the brain to begin the process. (9) Specifically, it induces selective activation in the nucleus paraventricularis, leading to erectogenic signals. (15)
It is this brain action that makes Uprima ® a unique new approach to the treatment of ED. As Dr. Dula stated after being involved with a trial of 1472 patients using Uprima ®; “From a urologist’s perspective, it is important to understand that this is an entirely novel agent and works totally differently to Sildenafil (Ed.- Viagra ®). It is a centrally-acting agent. What’s more, apomorphine works fairly quickly, in 15-25 minutes. The main side effect is nausea, but over time and repeated dosages it rapidly dissipates. We think that it is a safe and efficacious treatment for erectile dysfunction.” (19)
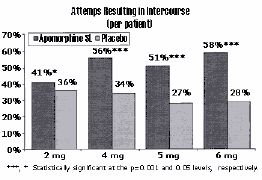
In a multi-center, double blind study (18), 520 patients (of an average median age of 54) took either 2mg, 4mg, 5mg, 6mg of apomorphine or a placebo. The number of attempts resulting in an erection firm enough for intercourse was recorded (Figure 4), along with the actual attempts resulting in intercourse. (Figure 5)
Figure 4
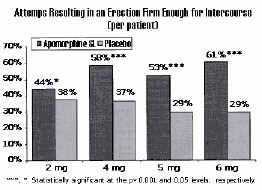
As can been seen from figures 4 and 5, the most significant improvements over placebo are at dosages of 4mg to 6mg. However it was clear in this same trial and others (9, 15, 16, 18), that increased dosages also increase the likelihood of the most common side effect of nausea. (Figure 6) These side effects are reported to diminish with continued dosing. (15)
Figure 5
In fact, the most favorable risk/ benefit ratio is seen with a dose optimization regimen of 3mg, with the 3mg dose providing efficacy comparable to that of 4mg, but with fewer side effects (15).
Other side effects with Uprima ® (9) include headache, dizziness, and flushing.
Figure 6
Contraindications with apomorphine include heart medications, (particularly those for hypertension) and because of potential synergy any other dopamine agonists such as bromocriptine, hydergine ®, deprenyl and L-dopa etc. Should you be taking such drugs, then always consult with your physician before embarking upon a concurrent use of apomorphine.
As stated earlier, the average dosages of Uprima ® are 2mg or 3mg taken sublingual (dissolved under the tongue) about 15 minutes before sex. (Note that the advent of the sublingual tablet is the only way that apomorphine should be used to treat ED). The drug insert clearly states, that (like most ED drugs), a 3mg dose should not be repeated again within any 8-hour period.
Conclusion:
Uprima ® represents a radical new departure in the treatment of ED. Rather than just stimulation to the penis for enhanced blood flow etc., for the first time brain receptor sites are being targeted for enhanced sexual performance.
I am confident that we are going to see other drugs being developed along similar lines in the coming months and years. I am also confident that similar (and even some of the same drugs), are eventually also going to be “approved” for sexual enhancement in females too.
References:
Related Products 4



